RETINA
MACULAR DEGENERATION RELATED TO AGE
Age-related macular degeneration (AMD) is the leading cause of uncorrectable low vision after age 60 in developed countries. AMD is more common in Caucasian patients.
It is responsible for a decrease in vision and / or the feeling of deformation of objects (wavy lines).
The precise causes of this disease remain unknown. The existing treatments only make it possible to slow down its evolution.
12% of the population between 65 and 75 years of age have AMD.
RISK FACTORS
age - the risk increases significantly from the age of 50
smoking
family history
high blood pressure
sun exposure significantly increases the risk
overweight
aspirin
ethnic origin
diet
DIAGNOSIS AMD
The diagnosis of the disease is established at the end of the assessment including at least an examination of the fundus, an OCT (optical coherence tomography).
Before considering treatment, fluorescein or infracyanin green (ICG) angiography is often necessary to distinguish between the different clinical forms of the disease.
There are two main forms of AMD:
the DRY form of AMD is an atrophy of the macula. There are only preventive treatments. This form represents 80% of AMD and the progression is slow. The affection is often bilateral.
the WET form represents 20% of AMD and corresponds to the appearance of new choroidal vessels (CNV). The wet form can be taken care of with repeated intravitreal injections (IVT).
TREATMENTS
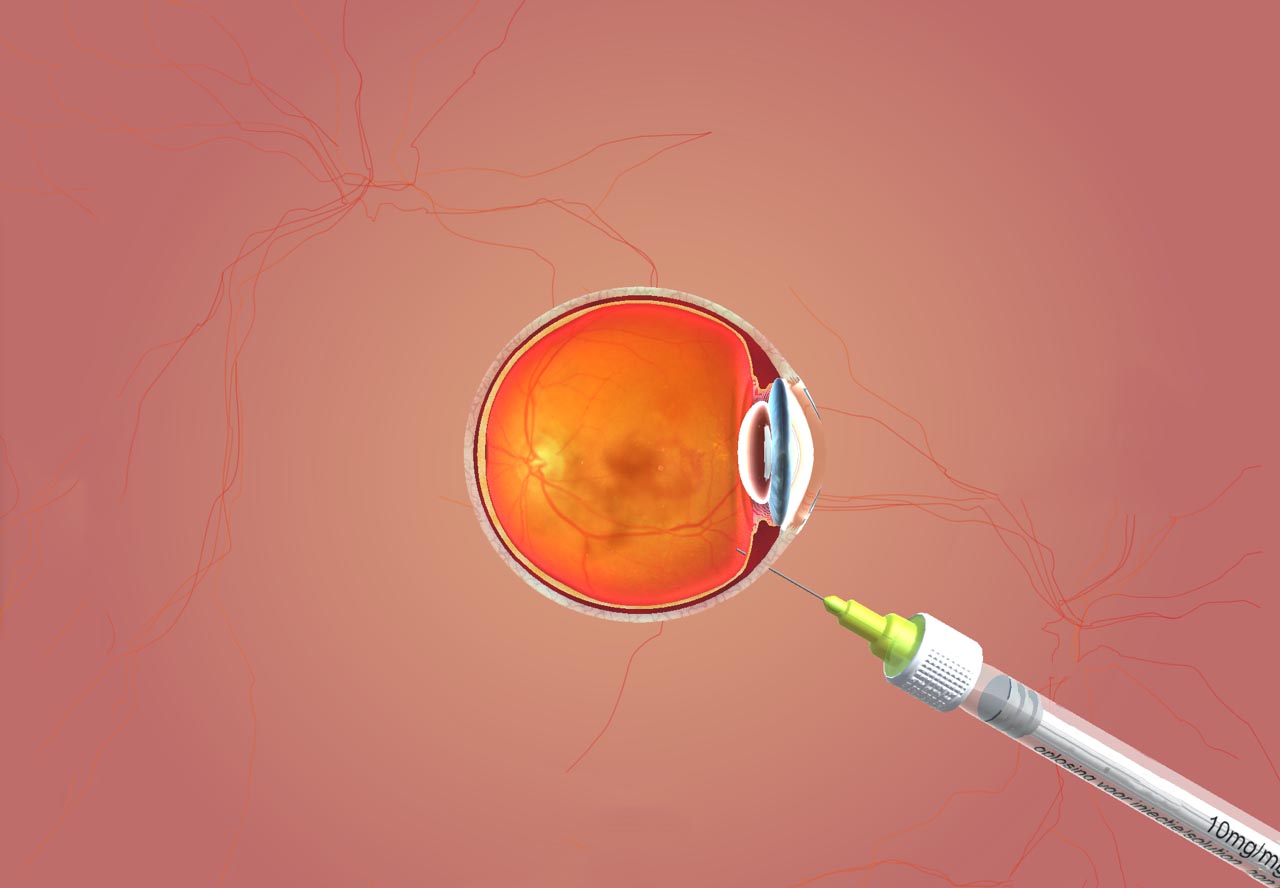
Two drugs are currently indicated in wet AMD: Lucentis® (Ranibizumab) used since 2007 and Eyelea® (Aflibercept) for which the marketing authorization is more recent. These two drugs are administered by intra-vitreous injection. These injections are performed under topical anesthesia and are very well tolerated. The most widely used treatment protocol includes a series of three monthly injections followed by a variable injection rate depending on the course of the disease observed during monitoring.
The surgeon performs IVT in outpatient care at CH Simone Veil de Vitré under topical anesthesia (anesthetic eye drops).
SURVEILLANCE
The surveillance of the disease includes the measurement of visual acuity, the examination of the fundus and especially OCT. Depending on these different elements, the continuation of the treatment or the abstention, and the monitoring, are decided at the end of each monitoring visit.
Self-monitoring must be performed by an Amsler grid.
DIABETIC RETINOPATHY
Diabetic retinopathy is a common complication of type 1 and 2 diabetes, affecting almost half of patients with diabetes for more than 15 years.
It is the leading cause of blindness in people under 60 and 30-40% of diabetic patients are carriers.
The main risk factors for the development of diabetic retinopathy are the type of diabetes (type 1> type 2), the duration of the diabetes and especially the glycemic balance (approximated by the measurement of glycated hemoglobin (HbA1c) .
Blood vessel abnormalities caused by diabetes can be made worse by certain associated factors such as high blood pressure and high cholesterol.
Depending on the importance and extent of retinal damage observed, diabetic retinopathy is classified into stages, which allows treatment to be tailored to the severity of the retinal disease.
In the absence of improvement in the risk factors of diabetic retinopathy and in the absence of treatment, it progresses to complicated forms.
DIABETIC RETINOPATHY SCREENING
Screening for retinopathy is done during the fundus examination, which requires pupil dilation. This examination must be repeated regularly, throughout the life of the diabetic patient, at a frequency which depends on the severity of the diabetes and the retinopathy, but also according to specific circumstances (pregnancy, modification of the hypoglycaemic treatment, postoperative monitoring. after cataract surgery, etc.…). In general, an annual check is recommended.
RETINOPHOTOGRAPHIES
If necessary, the fundus examination can be supplemented by retinophotographies, an examination of the macular zone by OCT (optical coherence tomography or Optical Cohérence Tomography) which makes it possible to analyze the retinal structures and to measure their 'thickness. OCT is essential for quantifying and monitoring macular edema.
RETINAL ANGIOGRAPHY
Retinal angiography may be necessary because it accurately assesses the state of the retinal vasculature. It is painless and lasts about fifteen minutes.
PREVENT DIABETIC RETINOPATHY
A satisfactory glycemic balance associated with control of the associated risk factors, which are arterial hypertension and hypercholesterolemia, constitute the essential elements of prevention.
TREATMENTS CURRENTLY USED
The laser is used to treat proliferative diabetic retinopathy (complicated by neo-vessels) and pre-proliferative. The goal of laser treatment is to photocoagulate the peripheral retina and achieve regression of the abnormal vessels.
Macular edema may benefit from treatment by intra-vitreous injection of an anti-VEGF substance (growth factor and blood vessel permeability). Repeated injections are necessary to maintain the benefit of the treatment.
If you want you can schedule an appointment
OR Call us on 09 86 34 99 22
Outside of practice opening hours and in case of emergency, please contact 15 or contact the CHU Pontchaillou in Rennes or the CH in Laval.
Doctor Laurentiu Popescu, ophthalmologist, consults at 6 Boulevard de Chateaubriant in Vitré in Ille-et-Vilaine.
Useful Links
National Council of the Order of Physicians French Society of Ophthalmology Ordinal compliance charter applicable to physician websites Legal Notice CNOM e-HealthAccess Map
OPHTALMO VITRE 36 Boulevard de Châteaubriant, 35500 Vitré, France
- Parking Gare de Vitré EFFIA nearby; Champ de Foire car park nearby - Bus nearby: Line 3 stop 70ème RI, Chateaubriant or Tremoille; line 7 Chateaubriant or Trémoille stop - Access to the SNCF train station on foot 400mContact
(+33) 09 86 34 99 22
https://www.ophtalmo-vitre.fr
LJ 9: 00-13: 00 and 14: 00-18: 00
V 9: 00-13: 00 and 14: 00-17: 00